}})
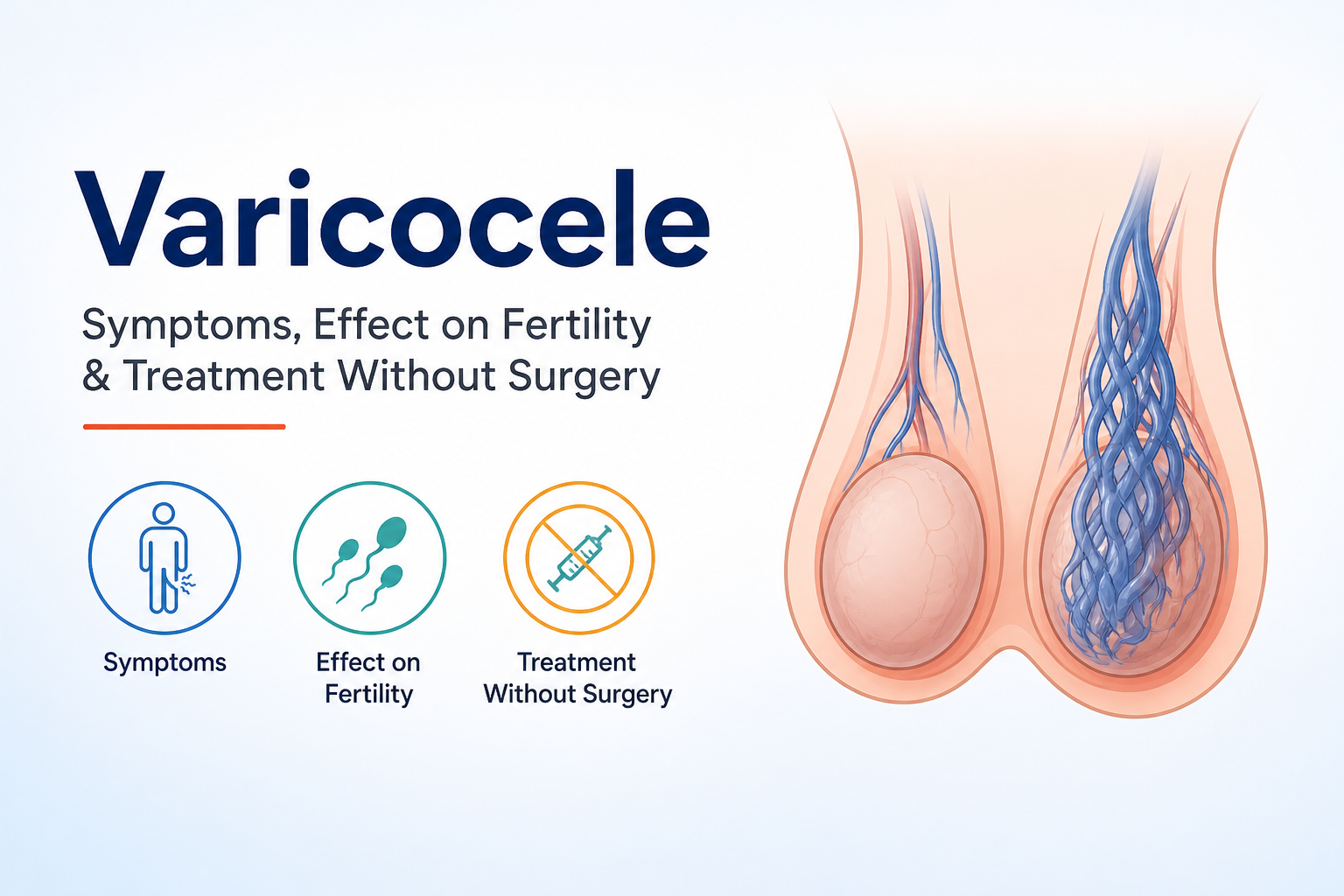
A varicocele is an abnormal enlargement of the veins inside the scrotum - the same type of problem that causes varicose veins in the legs, but located in the testicular venous network. When the one-way valves inside these veins fail, blood pools instead of draining efficiently back toward the heart. Over time, this pooling causes the veins to dilate, creating the characteristic "bag of worms" appearance that doctors look for during examination.
The condition can affect one or both testicles, though the left side is significantly more affected due to the anatomy of the left testicular vein and its angle of drainage into the renal vein.
What is a Varicocele?

Veins in the scrotum are designed to carry blood away from the testicles and back into the body's circulatory system. When the valves inside these veins malfunction, blood flows backward and collects in the vein. The resulting engorgement causes the vein to stretch and enlarge over time.
The consequence of this blood pooling goes beyond structural change. Pooled blood raises the local temperature inside the scrotum. The testicles are housed outside the body precisely because sperm production requires a temperature slightly cooler than the body's core. When scrotal temperature rises - even fractionally - the environment for sperm production becomes compromised.
This is the central mechanism through which varicocele damages fertility.
How Common Is Varicocele in Men?
- Varicocele affects approximately 15% of all men in the general population
- It is found in up to 40% of men presenting with infertility concerns
- It is the most common reversible cause of male infertility identified in clinical practice
- Most cases develop during puberty, though symptoms may not appear until adulthood
- Left-sided varicocele accounts for the majority of cases; bilateral varicocele is less common; right-sided varicocele alone is rare
Despite its prevalence, many men with varicocele have no symptoms and discover the condition only when investigating fertility difficulties.
Symptoms of Varicocele

Physical Symptoms
Not every man with a varicocele experiences discomfort, but when symptoms do occur, they typically include:
- A dull, aching pain or heaviness in the testicle - often worse after standing for long periods, physical exertion, or at the end of the day
- A visible or palpable mass in the scrotum - described as feeling like a "bag of worms" when palpated
- Scrotal heaviness or dragging sensation - particularly in warm weather or after activity
- Testicular atrophy - in some cases, the affected testicle shrinks in size over time due to impaired blood supply and hormonal disruption.
- Discomfort during or after physical activity - many men notice symptoms specifically during exercise or prolonged sitting.
Symptoms often improve when lying down, as this reduces the hydrostatic pressure on the scrotal veins.
When Varicocele Has No Symptoms
A significant proportion of varicoceles are completely asymptomatic. These are often discovered incidentally - during a routine physical exam, a fertility evaluation, or an ultrasound performed for another reason. The absence of pain does not mean the varicocele is harmless. Silent varicoceles can still impair sperm production and contribute to male infertility over time.
Grades of Varicocele

Clinicians classify varicocele into three grades based on size and detectability:
- Grade 1 - Small; only detectable by ultrasound or by the Valsalva manoeuvre (bearing down). Not palpable during a standard exam.
- Grade 2 - Medium; palpable on physical examination without Valsalva. Not visible through the scrotal skin.
- Grade 3 - Large; visible through the scrotal skin and easily palpable. The classic "bag of worms" presentation.
Grade 1 varicoceles detected only on ultrasound in men with normal sperm quality are typically monitored rather than treated. Grades 2 and 3, particularly when associated with fertility concerns or pain, are the most common candidates for intervention.
How Varicocele Affects Male Fertility

Scrotal Temperature and Sperm Production
The testicles sit outside the body because sperm production (spermatogenesis) requires a temperature approximately 2–4°C lower than core body temperature. The pooling of warm blood from the body's interior in dilated scrotal veins raises local scrotal temperature - disrupting this precisely regulated environment.
Even a small, sustained increase in scrotal temperature is enough to impair the delicate process of sperm maturation. This temperature effect is considered the primary mechanism linking varicocele to male infertility.
Impact on Sperm Count, Motility, and Morphology
The downstream effects of scrotal overheating manifest directly in semen quality. Men with varicocele typically show reductions across all three core semen parameters:
- Sperm count - fewer sperm are produced due to disrupted spermatogenesis
- Sperm motility - the ability of sperm to swim efficiently toward an egg is reduced
- Sperm morphology - the proportion of normally shaped sperm declines, making fertilisation more difficult
A semen analysis will often reveal these changes in men with clinically significant varicocele. Research has shown that successful varicocele treatment can raise average sperm count substantially, from approximately 2.4 million to 11.6 million per millilitre in some studies.
Varicocele and Testosterone Levels
Beyond fertility, varicocele can suppress testosterone production. The Leydig cells in the testicles - responsible for producing testosterone - are also sensitive to temperature and impaired blood flow. Men with varicocele may experience lower testosterone levels than expected for their age, contributing to reduced libido, fatigue, and diminished sexual function alongside infertility.
Diagnosing Varicocele
Diagnosis is typically a two-step process:
- Physical examination - A urologist or andrologist examines the scrotum while the patient is standing, both at rest and during a Valsalva manoeuvre. Grade 2 and 3 varicoceles are usually detectable this way.
- Scrotal ultrasound with Doppler - This is the gold-standard imaging tool. It confirms the diagnosis, grades the varicocele, detects reverse blood flow in the veins, and rules out other scrotal conditions. Grade 1 varicoceles are typically only found this way.
If fertility is the primary concern, a semen analysis will also be ordered to assess sperm count, motility, and morphology - helping determine whether the varicocele is affecting reproductive function.
Varicocele Treatment Without Surgery

Surgery is not the only answer. Several effective non-surgical and minimally invasive options exist, and for many men - particularly those with mild-to-moderate symptoms or early fertility concerns - they are entirely appropriate first choices.
Varicocele Embolization
Varicocele embolisation is the most clinically effective non-surgical treatment available and is considered equally effective to surgery in many cases. It is performed by an interventional radiologist - not a surgeon - typically as an outpatient procedure under local anaesthesia.
How it works: A thin catheter is inserted through a small incision in the groin or neck area and guided using imaging to the affected testicular vein. Small coils, foam, or a sclerosing agent are then introduced to block the vein, redirecting blood flow and eliminating the varicocele.
Advantages over surgery:
- No general anaesthesia required
- No surgical incision - only a small puncture site
- Shorter recovery time - most men return to normal activity within 1–2 days
- Comparable success rates to surgical varicocelectomy
- Lower risk of hydrocele (fluid accumulation) compared to surgical approaches
Men considering surgical treatment should always obtain a second opinion from an interventional radiologist to ensure they are fully informed about embolisation as an alternative. This option remains significantly underutilised despite strong evidence supporting its effectiveness.
Lifestyle Changes and Conservative Management
For men with mild varicocele, no fertility concerns, and manageable symptoms, conservative management is appropriate:
- Supportive underwear or a scrotal support (jockstrap) - reduces dragging discomfort and minimises blood pooling during physical activity
- Avoiding prolonged standing or heat exposure reduces symptom aggravation
- Over-the-counter pain relief - NSAIDs such as ibuprofen can manage mild discomfort on an as-needed basis
- Avoiding hot baths and tight clothing - minimises unnecessary scrotal temperature elevation
- Regular monitoring - periodic semen analysis and scrotal ultrasound to track whether the varicocele is progressing or affecting fertility over time
Conservative management does not repair the varicocele. It manages symptoms and slows deterioration, but it is not a standalone solution for men with fertility goals.
Nutritional Support and Antioxidants
Oxidative stress - driven by free radicals released by the damaged scrotal environment - is a key mechanism through which varicocele harms sperm DNA integrity. Antioxidant supplementation has shown promise in supporting sperm quality while definitive treatment is planned or managed conservatively:
- Coenzyme Q10 (CoQ10) - supports mitochondrial energy production in sperm cells
- Vitamin C and Vitamin E - neutralise oxidative stress in semen
- Zinc and Selenium - essential minerals for healthy spermatogenesis
- L-Carnitine - supports sperm motility and energy metabolism
- Folic acid - supports sperm DNA integrity
These supplements do not treat the varicocele itself but can support better semen parameters during the period before or instead of definitive treatment.
When Surgery (Varicocelectomy) Becomes Necessary
Non-surgical management has clear limits. Varicocelectomy - the surgical repair of a varicocele - becomes the recommended option when:
- Fertility is the primary goal, and semen parameters are significantly impaired
- The varicocele is Grade 2 or 3 with confirmed fertility impact
- Pain is persistent and disabling and has not responded to conservative measures
- Testicular atrophy is progressing, particularly in adolescents, where future fertility must be protected
- Embolisation has failed or is anatomically not feasible
- The couple has unexplained infertility, and the male partner has a detectable varicocele
Varicocelectomy is typically performed as an outpatient procedure. The most precise approach - microsurgical subinguinal varicocelectomy - uses a surgical microscope to tie off the affected veins with minimal risk to surrounding structures. Recovery takes approximately 2–4 weeks.
Does Treating Varicocele Actually Improve Fertility?
The evidence is encouraging but nuanced.
- Studies show that varicocele treatment improves semen parameters in the majority of men who undergo it.
- Sperm count, motility, and morphology all tend to improve following successful repair.
- Natural conception rates increase after treatment, though they do not reach 100% - fertility depends on multiple factors, including the partner's reproductive health.
- Treatment is most effective when the varicocele is clinically detectable (Grade 2 or 3) and when semen parameters are abnormal before treatment.
- Varicoceles detectable only by ultrasound in men with normal sperm quality have not been shown to benefit significantly from treatment.
The decision to treat should always be made in consultation with a urologist or reproductive specialist who can assess individual semen parameters, varicocele grade, the partner's fertility status, and overall reproductive goals.
Expert Tips for Managing Varicocele
These insights reflect what genuinely helps men navigate a varicocele diagnosis more effectively:
- Get a semen analysis first, always. A varicocele diagnosis without a semen analysis is incomplete. The results tell you whether the varicocele is functionally affecting your fertility - and that answer determines the urgency and type of treatment needed.
- Ask about embolisation before booking surgery. Many men are referred directly to surgeons without being told that embolisation exists. Ask your GP or urologist for an interventional radiology opinion - it is a legitimate, equally effective alternative with faster recovery.
- Do not wait indefinitely. Varicocele causes progressive damage over time. Testicular function tends to decline the longer the condition is left untreated in men with fertility concerns. Monitoring is appropriate for mild cases but should not replace timely action when parameters are declining.
- Treat fertility as a couple's issue. A female partner's age and reproductive health directly influence how aggressively a varicocele should be treated. If the female partner is over 35, time is critical - your specialist should factor this into the treatment timeline.
- Manage heat proactively. Whether or not you choose treatment, reducing scrotal heat load - avoiding hot baths, saunas, tight underwear, and prolonged sitting - is a low-cost, evidence-supported way to protect sperm quality in the interim.
Conclusion
Varicocele is the most common reversible cause of male infertility - yet it is frequently underdiagnosed, misunderstood, and poorly explained to the men who have it. The good news is that effective pathways exist at every stage, from conservative management for mild cases to highly effective non-surgical embolisation for those requiring intervention.
Key takeaways:
- Varicocele is an enlargement of scrotal veins that raises testicular temperature and impairs sperm production
- Symptoms range from no symptoms at all to scrotal pain, heaviness, and testicular atrophy
- It is found in up to 40% of infertile men and is the most common reversible male infertility cause
- It damages sperm count, sperm motility, and sperm morphology through heat and oxidative stress
- Non-surgical treatment - especially varicocele embolisation - is as effective as surgery with fewer risks and faster recovery
- Lifestyle changes and antioxidant support can assist management in mild cases.
- Surgery remains the appropriate choice for severe, progressive, or fertility-critical cases.
If you have been diagnosed with a varicocele, or you suspect one, the smartest next step is a semen analysis and an appointment with a urologist or fertility specialist who presents all your options - not just one.