}})
You finish a course of antibiotics. The burning stops. You feel better. Then, three weeks later, it comes back - and so does the frustration.
If this cycle sounds familiar, you are not alone. Millions of people, particularly women, experience repeated urinary tract infections every year. But here is a question most doctors do not ask: are these actually new infections, or is the same infection simply refusing to go away?
That distinction matters more than you might think. Whether you have a chronic UTI or a recurrent UTI determines how your condition should be tested, treated, and prevented. Getting it wrong can mean years of ineffective treatment, growing antibiotic resistance, and unnecessary suffering.
This guide explains both conditions clearly - what causes them, why standard treatment often fails, what science says about the underlying biology, and what you can do about it right now.

What is a Recurrent UTI?
A recurrent urinary tract infection (UTI) is defined as experiencing two or more UTIs within a six-month period, or three or more within a single year. You may also hear it called a frequent UTI, persistent UTI, or chronic UTI - though these terms are not always used consistently, even by healthcare providers.
Recurrent UTIs are more common than most people realize. Over 50% of women will have at least one UTI in their lifetime. Of those, about 26% will experience a recurrence within six months of the first infection. Risk increases with every additional episode.
Official Definition and Frequency Thresholds
When a healthcare provider identifies recurrent UTIs, they look for one of two patterns:
- Two or more UTIs within six months
- Three or more UTIs within twelve months
This definition tells you how often the infections occur. What it does not tell you is why - and that missing piece changes everything about how you should be treated.
What Is a Chronic UTI?
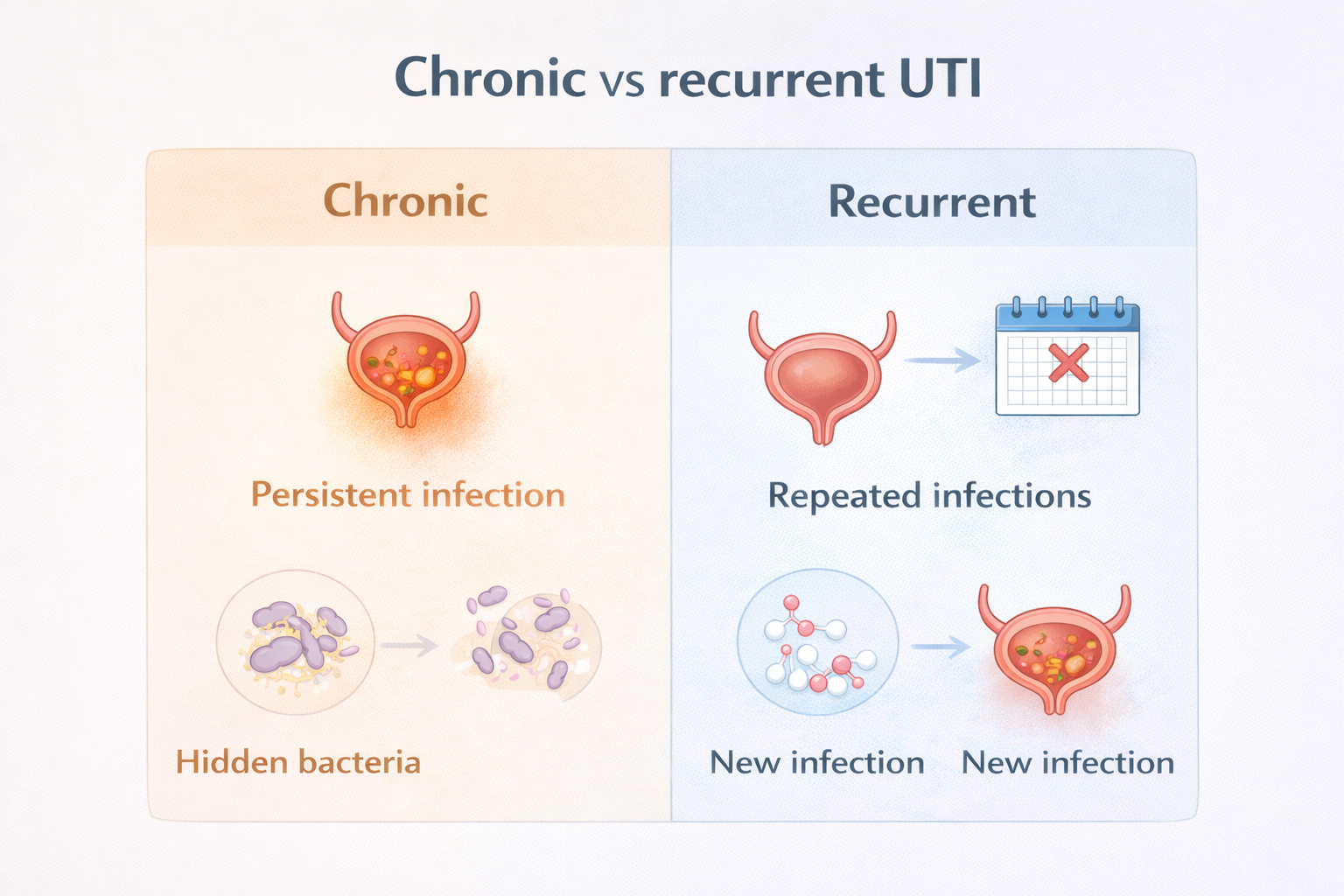
A chronic UTI - also called chronic cystitis - is a persistent bladder infection where the original bacteria were never fully cleared. Rather than a new infection entering from outside, a chronic UTI is one that quietly remains in the bladder even after antibiotics appear to resolve the symptoms.
This is a subtle but critical distinction. Many cases labeled as recurrent UTIs are actually a single, ongoing chronic infection that dipped below what standard tests can detect, then flared back up. Frequent UTIs caused by an underlying persistent infection are also referred to as chronic cystitis or chronic bladder infection.
Reinfection vs Relapse - The Distinction That Changes Everything
Medical providers separate recurrent UTI cases into two categories:
- Reinfection - A genuinely new infection caused by the same or different bacteria entering the bladder after the previous one was fully cleared.
- Relapse - The same bacteria reappear within two weeks of completing treatment, indicating the original infection was never fully eradicated. This points to a persistent or chronic UTI.
Most recurrent UTIs diagnosed in primary care are classified as reinfections. However, growing research suggests that a significant proportion of these cases are actually relapses - chronic infections that standard testing simply cannot detect.
Understanding which one you have is the first step toward getting the right care.
Why Do I Keep Getting UTIs? The Biofilm Explanation
If your UTIs keep returning despite completing antibiotics, staying hydrated, and following every hygiene recommendation, there is a biological explanation that mainstream medicine has been slow to address: biofilms.
The National Institutes of Health (NIH) estimates that around 80% of all bacterial infections in humans involve biofilms. Yet standard UTI testing does not screen for them.
How Biofilms Form in the Bladder
A biofilm is a structured community of bacteria that attaches directly to the bladder wall and produces a protective coating - sometimes described as a slime shield - that antibiotics and your immune system struggle to penetrate.
Here is how the process typically unfolds:
- Bacteria enter the bladder and initially float freely in urine
- They begin attaching loosely to the bladder lining
- Over time, they form a strong, organized colony on the bladder wall
- The colony produces a protective extracellular matrix (biofilm)
- Antibiotics kill the free-floating bacteria but cannot fully penetrate the biofilm
- The biofilm community survives and eventually re-seeds the bladder
Bacteria can also burrow inside the actual cells of the bladder wall, forming what researchers call intracellular bacterial communities (IBCs). These are even harder to detect and treat. Evidence of IBCs has been found in approximately one in five urine samples from women with symptomatic UTIs.
The Flare-Up Cycle Explained
The biofilm is not static. It periodically releases bacteria back into the urine - and that is precisely when symptoms flare. This explains the pattern many chronic UTI sufferers recognize: a period of acute, painful symptoms, followed by relative calm, then another sudden flare.
The cycle typically works like this:
- Bacteria escape the biofilm and enter the urine
- The immune system detects the threat and triggers inflammation
- Burning, urgency, and frequency symptoms appear
- Antibiotics or the body's defenses clear the free-floating bacteria
- Symptoms ease - but the biofilm remains intact on the bladder wall
- The biofilm regenerates and eventually releases bacteria again
- Symptoms return and are often misread as a brand-new infection
This cycle can repeat indefinitely. That is why for many people, each course of antibiotics provides short-term relief but never resolves the underlying problem.
Symptoms of a Chronic or Recurrent UTI

The symptoms of a chronic UTI or recurrent UTI are largely the same as a typical acute infection, but may fluctuate in intensity over time. Common symptoms include:
- Burning or pain when urinating (dysuria)
- Frequent or urgent need to urinate
- Pressure or pain above the pelvis (suprapubic pain)
- Cloudy or foul-smelling urine
- Blood in the urine (hematuria)
- Feeling that you cannot fully empty your bladder
- Urinary leakage (urinary incontinence)
Some people with a chronic bladder infection experience low-level, constant symptoms between flares - a nagging urgency or mild discomfort that never fully disappears. Others have clear periods between acute episodes, making it appear as though a new infection has struck each time.
Important: If you develop fever, back pain, chills, or nausea alongside these symptoms, seek medical care promptly. These can signal that the infection has reached the kidneys (pyelonephritis), which requires urgent treatment.
Risk Factors You Should Know About
Several factors can increase your risk of developing chronic or recurrent UTIs. Understanding yours can help you and your doctor target the right interventions.
Anatomical and medical factors:
- Vaginal atrophy (atrophic vaginitis), particularly after menopause or cancer treatment
- Bladder diverticula - pockets in the bladder wall that trap urine and bacteria
- Incomplete bladder emptying (urinary retention) caused by diabetes, stroke, or neurological conditions
- Kidney stones or structural urinary tract abnormalities
- Vesicoureteral reflux (VUR)
Hormonal factors: After menopause, falling estrogen levels reduce vaginal acidity, decrease protective Lactobacilli bacteria, and weaken the bladder muscles - creating ideal conditions for bacterial overgrowth and bladder infection. Postmenopausal women face a significantly higher risk of recurrent lower urinary tract infection.
Behavioral and lifestyle factors:
- Use of spermicides or diaphragms, which disrupt the vaginal microbiome
- High frequency of sexual intercourse (more than twice weekly triples UTI risk)
- Wiping back to front after using the toilet
- Low daily fluid intake
- Prolonged intervals between urination
- Taking baths rather than showers
Genetic predisposition: If your mother or sister has a history of frequent UTIs, you are at higher risk due to inherited differences in how bacteria adhere to urinary tract tissue.
How Are These Conditions Diagnosed?
For most patients with recurrent UTIs, standard diagnosis involves a urinalysis and urine culture. The American Urological Association (AUA) recommends obtaining both with each episode of acute cystitis.
Urological imaging - such as a renal ultrasound or CT scan - is generally reserved for specific scenarios, including relapsing infections, persistent blood in the urine after treatment, recurrent kidney stones, or repeated isolation of certain bacteria like Proteus, which is associated with stone formation.
Why Standard Urine Cultures Often Fail
Here is a problem most patients are never told about: standard urine cultures are designed to detect free-floating bacteria in the urine. They are not designed to detect biofilms or IBCs embedded in the bladder wall.
This means that even when a significant chronic infection is present, standard testing can return a negative result - leading to a diagnosis of "no infection found" when an infection clearly is present. This gap in testing accuracy has led to many people being misdiagnosed with Interstitial Cystitis (IC) or Painful Bladder Syndrome (PBS) - both diagnoses of exclusion given when no cause can be identified.
Research suggests that some newer testing approaches, such as DNA sequencing of urine samples, can detect microorganisms regardless of whether they are free-floating or embedded in a biofilm. These tests are not yet widely available, but awareness of their existence can help you advocate for more thorough evaluation.
Treatment Options - From Antibiotics to Natural Strategies

Treatment of chronic and recurrent UTIs should ideally follow a clear path: test, diagnose, treat, evaluate, and prevent. In practice, many patients cycle through repeated short courses of antibiotics without ever addressing the underlying cause.
Antibiotic Prophylaxis
When conservative measures are not enough, long-term low-dose antibiotic prophylaxis is considered the gold standard for recurrent UTI prevention. Options typically include:
- Nitrofurantoin (50–100 mg daily at bedtime)
- Sulfamethoxazole-trimethoprim (SMX-TMP) at low dose
- Trimethoprim (100 mg daily at bedtime)
- Cephalexin (125–250 mg daily at bedtime)
For women whose UTIs are clearly linked to sexual activity, post-coital prophylaxis - taking a single antibiotic dose after intercourse - is an effective and targeted alternative to continuous daily dosing.
Long-term antibiotic use carries its own risks, including disruption of the gut and vaginal microbiome, yeast overgrowth, and the promotion of antibiotic resistance. This is why non-antibiotic strategies are increasingly recommended as first-line prevention.
Non-Antibiotic and Natural Approaches
Several non-antibiotic options have shown promise in reducing recurrent UTI episodes:
- Vaginal estrogen therapy - For postmenopausal women, this is one of the most effective preventive treatments available. Applied as a cream, tablet, or ring directly in the vagina, it restores local acidity and Lactobacilli populations. Minimal estrogen enters the bloodstream.
- Cranberry supplements - Contain proanthocyanidins that may reduce bacterial adhesion to the bladder lining. Evidence remains mixed on cranberry juice, but concentrated supplements appear more promising.
- D-mannose - A naturally occurring sugar thought to bind to bacteria and prevent them from adhering to the urothelium. Commonly suggested at 500 mg twice daily, though optimal dosing is still under research.
- Methenamine hippurate - Acidifies the urine to create an environment that inhibits bacterial growth. A recent systematic review found it effective and well-tolerated as a prophylactic agent.
- Increased hydration - A clinical trial of 140 women found that increasing daily water intake to at least 1.5 liters reduced UTI episodes by an average of 1.5 fewer infections per year compared to controls.
- Probiotic support - Lactobacillus-based probiotics may help restore the vaginal microbiome, though current evidence from clinical trials remains inconclusive.
Prevention Tips You Can Start Today

Many recurrent UTIs can be reduced - and sometimes eliminated - with consistent changes to daily habits. Here is what you can do on your own:
- Always wipe from front to back after using the toilet
- Drink at least 1.5 to 2 liters of water daily
- Urinate within 30 minutes after sexual intercourse
- Avoid spermicides and switch to an alternative contraception if needed
- Urinate regularly and do not hold your bladder for extended periods
- Take showers instead of baths
- Use a gentle liquid soap for cleaning the urethral area, and clean that area first
- If you are postmenopausal, ask your doctor about vaginal estrogen cream
- Wear breathable, loose-fitting underwear
- Avoid prolonged cycling or horseback riding, which can introduce bacteria into the urethra
When to See a Doctor
See a healthcare provider promptly if:
- You have had more than two UTIs in the past six months, or more than three in the past year
- Your symptoms do not clear within 48 hours of starting antibiotics
- You have continuous urinary symptoms, but have never received a clear diagnosis
- You have been diagnosed with Interstitial Cystitis, but want a second opinion on whether an infection may be present
- You develop fever, back pain, chills, or vomiting alongside urinary symptoms - go to the emergency room
If you have seen a primary care provider repeatedly without resolution, ask for a referral to a urologist or urogynecologist who specializes in complex or recurrent lower urinary tract infections. Specialists in this area can access more advanced testing and longer-term treatment protocols.
Conclusion
The difference between a chronic UTI and a recurrent UTI is not just a matter of medical labels. It is a distinction with real consequences for how your condition is treated, whether it improves, and how much of your life is spent managing symptoms that could potentially be resolved.
Key takeaways:
- A recurrent UTI is defined by frequency (2 in 6 months or 3 in a year); a chronic UTI refers specifically to a persistent, never-fully-cleared infection
- Many apparent reinfections are actually relapses - the same bacteria surviving in a biofilm on the bladder wall
- Standard urine cultures do not detect biofilms, which is why many chronic UTI cases go undiagnosed
- Effective prevention combines hygiene habits, hydration, and - where appropriate - vaginal estrogen or targeted antibiotic prophylaxis
- Non-antibiotic options, including cranberry supplements, D-mannose, and methenamine hippurate, offer viable alternatives worth discussing with your doctor
- You do not have to accept repeated infections as simply your fate - better testing and treatment exist
Talk to a specialist. Ask better questions. And do not stop advocating for yourself until you get real answers.